Dr Brenda Baker BDS (Hons.) Syd MSc. (London) Clinical and Technical Consultant Southern Cross Dental and Modern Dental Pacific.
Confusion sometimes exists with some clinicians regarding the choice of materials to employ in clinical situations. This summary article outlines guidelines for various materials available and preparation principles. The underlying composition of dental ceramics determines their physical properties which will, accordingly, dictate their suitability for any given clinical situation. Consider dental ceramics as a spectrum with an unfilled glassy matrix at one end and a virtually wholly crystalline structure with little if any matrix at the other end.
Feldspathic Ceramics (Glass Matrix)
These are largely vitreous or glass ceramics, with 3D networks of atoms having no regular pattern to the spacing and characterised by an amorphous structure.
Glass-Based Ceramics (Filled particles)
Filler particles are added in increasing amounts to the base glass matrix to improve mechanical properties and to control optical effects such as opalescence, colour and opacity. The first fillers to be used contained particles of a crystalline mineral called leucite. This was added by simply mixing in the filler ceramic (between 17-25% mass). The porcelains created could be fired successfully onto metal substructures. An alternative approach is where the f iller particles are grown inside the basic glass restoration after it has been formed. In one approach, the glass is given a special heat treatment (ceraming), causing the precipitation and growth of the crystals within the glass. The fillers are derived chemically from atoms of the glass itself.
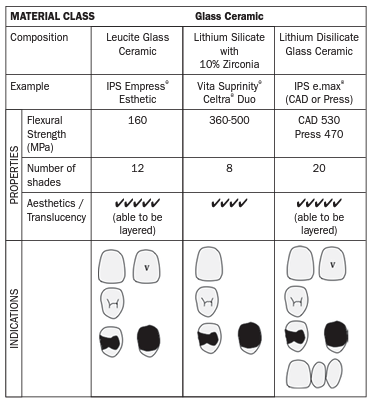
Examples of glass-based ceramics include IPS e.max®, IPS e.max® ZirPress and Vita Suprinity®. IPS e.max® is a 70% lithium disilicate glass ceramic which offers:
- Optimised translucency – light diffusion properties.
- Pleasing aesthetics u superior durability (470-530 MPa flexural strength).
- Strength for full anatomical restorations.
- Opalescence.
- Option of monolithic (solid) aesthetic restorations using CAD, or layered/veneered restorations for optimum aesthetics
Clinical Tip for use of IPS e.max®:
- Crowns – anterior & premolar.
- Inlays/onlays.
- Veneers.
- Anterior implant crowns.
- Anterior 3-unit bridges (include premolar) – Use Press ONLY.
Clinical Tip for IPS e.max®
Bridges In the anterior region (up to canine) the pontic width should not exceed 11mm. In the premolar region (canine to second premolar) the pontic width should not exceed 9mm.
Bridges of more than 3 units or those in the premolar to molar region should instead be fabricated as IPS e.max® ZirPress.
Clinical Tip for IPS e.max® ZirPress
Consider using IPS e.max® Ceram pressed over zirconium oxide substructures for patients with bruxism or where the span length or tooth size prevents ideal use of IPS e.max®. The porcelain used can be matched to adjacent IPS e.max® crowns. When stump shade is dark, consider using a more opaque ingot. There are different values and hues of the ingots. Allow adequate preparation depth for the zirconia structure and overlying porcelain.
Suitable for:
- Single-tooth restorations.
- Bridges in the anterior and posterior region.
- Implant superstructures
VITA SUPRINITY® is a millable lithium silicate glass ceramic with 10% zirconia.
High-Strength Crystalline Ceramics
Polycrystalline ceramics contain densely packed atoms with little or no vitreous glassy ‘matrix’ phase.
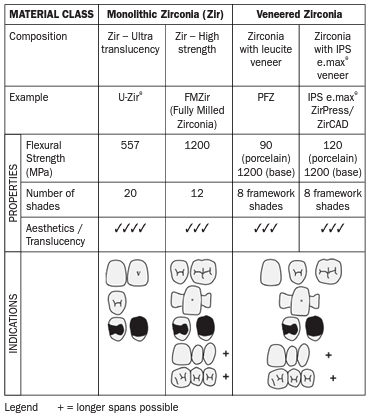
Polycrystalline ceramics are more opaque and more difficult to process into complex shapes than glass ceramics. Computer-aided manufacturing (CAM) has allowed well-fitting prostheses made from polycrystalline ceramics to become possible. Zirconia is the commonest example of polycrystalline ceramics and can be either monolithic (unlayered or “fully milled”) or layered with a veneering ceramic, which is called porcelain-fused-to-zirconia (PFZ).
A. Monolithic Fully Milled Zirconia (FMZ)
Considerations when using Monolithic Zirconia:
- FMZ crowns can readily mask out discoloured, non-vital teeth where sufficient tooth preparation exists of at least 0.6 mm.
- Thicknesses greater than that are far too opaque for upper anteriors.
- Overpreparation of teeth is contraindicated when using monolithic zirconia as there is no need to create room for veneering porcelain.
FMZ restorations are coloured utilising a three-zone colouring system while in the unsintered state:
- The restoration is brushed with the final shade around the cervical area.
- The desired body shade is then applied.
- Effect shades are finally added to the occlusal aspect.
Clinical Tips for Zirconia Restorations
- With adequate connector size, 3-, 4- and even 6-unit bridges are very dimensionally predictable. Consider “closed” embrasures in the design to allow sufficient connector bulk.
- After trying-in the restoration and checking fit and occlusion, the fitting surface needs to be disinfected then cleaned to remove all contaminants. This can be achieved with Ivoclean™ although sandblasting with up to 50 micron abrasive is also effective (Powers, J.M., et al., 2009). The restoration should then be rinsed and dried.
- Zirconia should never be etched as this will impair bonding especially where phosphoric acid is used.
UZir Ultra Translucent is a new formula of zirconia, offering a unique combination of translucency and strength. This product is a breakthrough given that traditionally zirconia is considered a strong but opaque material with questionable aesthetics in anterior regions. The strength of UZir is higher than more translucent alternatives and so it addresses the market in between glass ceramics and the more opaque crystalline zirconias. Multi-layered blocks enhance aesthetics without compromising strength by layering.
Translucency is similar to IPS e.max®.
Clinical Tip for UZir:
Consider ultra translucent zirconia for cases where strength and resistance to chipping are required in combination with good aesthetics.
Suitable for anterior crowns, inlay/onlays and other single unit restorations, some posterior crowns.
B. Porcelain-fused-to-Zirconia
- Used as a more aesthetic option than monolithic zirconia.
- Zirconia forms the framework material for anterior and posterior crowns and bridges, with veneering porcelains applied over all or part of this zirconia core.
- Veneering porcelains have evolved with fine microstructures with improved optical properties and clinical performance. They are more translucent and generally produce excellent aesthetics in 0.6 mm thickness (over a 0.6 mm zirconia coping) meaning a reduction of at least 1.2 mm is critical.
- More tooth preparation is needed than for FMZ to allow room for veneering porcelain.
Clinical Tip
Core bulk fractures in bridges with PFZ or monolithic zirconia are most commonly located in the connector region and start from the gingival surface upward where the tensile forces are greatest due to occlusal loading.
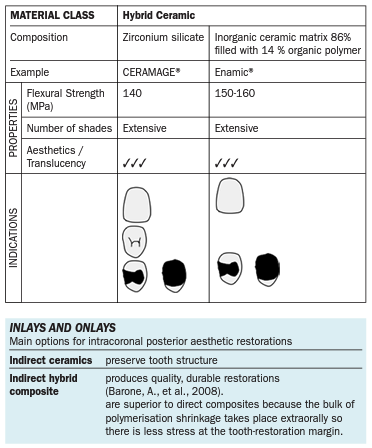
Hybrid Ceramics
These are considered “high performance polymers”. The materials are composite materials which contain either ceramics, nanoceramics or glass combined with different resin components. They can be used for either temporary or permanent restorations. Commonly used materials are CERAMAGE® and Enamic®.
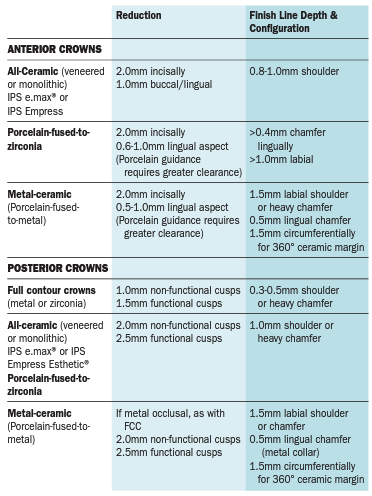
Suggested Preparation Features for Crowns
Evaluate:
- Coronal support
- Axial wall preparation – Two-plane buccal reduction of anterior teeth.
- Tooth reduction on incisal/occlusal surfaces – even reduction, depth grooves.
- Tooth form – ensure circumferential irregularity
- Total occlusal convergence – ideal TOC should be between 10-22°.
- Tooth height – anterior teeth 5 mm; posterior teeth 4 mm.
- Margin design – NO knife edge margins for all-ceramic restorations.